Full Text Article Open
Access 
Case report
Surgical repair of perimembranous ventricular septal defect and aortic regurgitation in an adult patient with Laubry-Pezzi syndrome.
Riache Abir1,2, *, Kebour Djamal
1,2, Sayah Toufik
1,2.
|
1: Department
of cardiothoracic surgery Military hospital of Algiers, Algeria 2: Medical University of Algiers, Algeria * Corresponding author Correspondence to: head1tech@gmail.com Publication Data: Submitted: September 22,2019 Accepted: December 12,2020 Online: March 15,2020 This article was subject to full
peer-review. This is an open access
article distributed under the terms of the Creative Commons Attribution Non- Commercial License 4.0 (CCBY-NC) allowing sharing and
adapting. Share: copy and redistribute the material in any medium or format. Adapt: remix, transform, and build upon the licensed material. the work provided must be properly cited and cannot be used for commercial purpose. |
Abstract |
|
Laubry-Pezzi syndrome is a congenital heart disease that consist
in a prolapse of aortic
valve cusping into
a subjacent ventricular septal defect due to Venturi effect. It results in progressive aortic valve insufficiency. The perimembranous type is the most common due to the proximity of the aortic
annulus to such
defects. The aim of this report is to highlight the specificity of the diagnosis and the surgical management of this
syndrome in adult
patients. Keywords: Laubry-Pezzi syndrome; aortic regurgitation; ventricular septal defect; surgery. |
|
|
Introduction Laubry and Pezzi
first described
the association of ventricular septal defect (VSD) and aortic regurgitation (AR)
in 1921. The
syndrome is a congenital heart insidious disease. The management of this rare pathology is still non-consensual regarding operative timing and techniques. The early
diagnosis of the VSD is capital
before the appearance of AR. Few cases of Laubry-Pezzi syndrome have been reported in the literature mostly in children [1,2]. we report
a case of Laubry-Pezzi syndrome in an adult patient managed in our cardiovascular surgery
department. Observation We report
the case of 32-year-old man patient with a previously asymptomatic ventricular septal defect (VSD) presented with New York Heart
Association class II symptoms and signs
of severe aortic insufficiency. The echocardiography showed perimembranous ventricular septal
defect VSD 7mm and severe aortic
regurgitation. The right
ventricular (RV) WAS 52 mmHg denoting of pulmonary hypertension (figure 1). The Laubry
Pezzi syndrome was diagnosed and surgery was indicated. A median
sternotomy incision was performed. The Cardiopulmonary bypass was established using
bicaval cannulation, and moderate hypothermia. After
aortic cross clamping, the ascending aorta was opened
through an oblique incision allowing an access
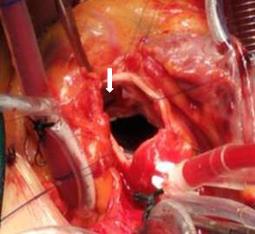
in an “trans-aortic approach”. The intraoperative findings were confirmed by inspecting the aortic sinuses and elevating the right coronary cusp. There was a perimembranous VSD and prolapsed aortic valve in the right
coronary cusp. We closed
the VSD using interrupted, pledgeted horizontal mattress sutures
(figure2). The procedure is completed by a free
margin placating of the right
coronary cusp. This
reduction of the free edge of the right coronary cusp elongated and
repositioned the hinge point of the right
coronary cusp
to restore the normal height
of the cusp,
hence a normal
surface of apposition. The procedure was verified by a post bypass
intraoperative transesophageal echocardiography. |