
Full Text Article Open
Access 
Case report
Strangulated Morgagni hernia
and sliding hiatal
hernia: A rare association.
Ferjaoui Wael 1,2*, Karouia Souhaiel1,2, Talbi Ghofrane1,2, Gabsi Soufien1,2, Bayar Rached1,2, Khalfallah Mohamed Tahar1,2.
|
1: Department of general surgery
Mongi Slim Hospital Tunis Tunisia 2: College of medicine Tunis Tunisia * Corresponding author Correspondence to: Publication Data: Submitted: September12,2019 Accepted: January 30, 2020 Online: March 15, 2020 This article was subject to full
peer-review. This is an open access
article distributed under the terms of the Creative Commons Attribution Non- Commercial License 4.0 (CCBY-NC) allowing sharing and
adapting. Share: copy and redistribute the material in any medium or format. Adapt: remix, transform, and build upon the licensed material. the work provided must be properly cited and cannot be used for commercial purpose. |
Abstract |
|
Morgagni hernias are congenital diaphragmatic hernias accounting for 3 to 5% of all diaphragmatic hernias. The association with
hiatal hernia
is rarely
reported in the literature. We report another case of a right Morgagni hernia revealed by an acute intestinal obstruction associated with a sliding hernia hiatal. The aim is to discusses the clinical presentation and to highlight the management characteristics. Keywords: Morgagni Hernia; Hiatal Hernia Type I; intestinal obstruction; surgery. |
|
|
Introduction The diaphragm muscle has some
weak spots giving
rise to hernias. Morgagni type is the organ
herniation through the para-retrosternal hiatus.
It represents 3-5%
of all diaphragmatic Hernias and occurs
mostly on the right
side [1]. Hiatal
hernias with
the protrusion of a portion
of the stomach
into the thoracic cavity are the most common. The association of these
hernias in the same patient remains exceptional. Only a few cases
have been described in the literature [2]. Observation A 75-year-old female patient with
no pertinent past
medical history presented to our emergency department with acute abdominal pain and recurrent episodes of vomiting. On physical examination, she was apyrexial and vitally stable. Abdomen
was distended and
tender. Breath sounds were decreased
on the
right side of the chest.
The abdomen X- ray erect showed
multiple differential air-fluid levels. The chest
radiography showed
an air-fluid level in the right side of mediastinum (figure 1). A computed tomogram (CT) of the chest and the abdomen revealed a Morgagni hernia through a retrosternal right diaphragmatic defect with protrusion of the transverse colon and a part of the great
omentum. A sliding hiatal
hernia was simultaneously discovered with visualized partially protruded stomach in the thoracic cavity (figure 2). |

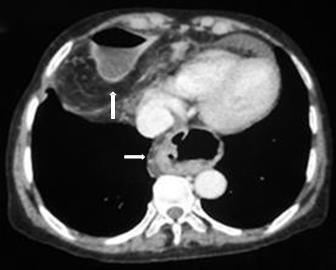
Figure 1: Chest
x-ray revealing a mediastinal air-fluid level Figure 2: Computed
tomography showing
coexistence of both hernias
The patient underwent midline laparotomy. Intraoperative findings were in favor of a defect in the diaphragm measuring 5*4 cm. This defect is located in the right side of the retrosternal region. The hernia contained the transverse colon and omentum with stricture effect causing bowel obstruction and dilatation. The adhesions were released. The contents were reduced into the abdomen. The diaphragmatic defect was repaired using non resorbable sutures (figure 3). The repair of the hiatal hernia was postponed for further endoscopic investigations. The postoperative courses were uneventful. The post-operative chest x-ray was unremarkable. The patient was discharged on the 4th day after surgery.

A B C
Figure 3
A: Intraoperative features of diaphragmatic hernia with herniated
omentum and transverse colon. B: Intraoperative features of Morgagni’s hernial
defect.
C: repair of the
defect using non resorbable sutures
Discussion
The coexistence of two non-traumatic diaphragmatic hernias is an extremely rare clinical condition. Only few cases have been previously reported since 1958. Morgagni hernia is a congenital diaphragmatic hernia that occurs through the parasternal hiatus of the diaphragm. It is more often right sided (90%) but it can be left sided (2%) or even bilateral (8%) [3,4]. Morgagni hernia is usually asymptomatic and has insidious evolution. Otherwise presenting symptoms may include chest or abdominal pain, dyspnea, dysphagia, or respiratory distress. The diagnosis is made incidentally or at the moment of complications in more than 30% of cases [5]. Our patient developed intestinal obstruction due to colon incarceration. The chest and abdomen computed tomography is the is more accurate for the diagnosis specially for asymptomatic patients [6]. The sliding hiatal hernia (type I) is a non-traumatic acquired hernia characterized by protrusion of the gastroesophageal junction into the posterior mediastinum through the esophageal hiatus. The association of these two hernias is uncommon and usually reported in adult patients [7]. The presence of a diaphragmatic hernia reduces the intra-abdominal pressure and might decrease the likelihood of a second diaphragmatic hernia formation. Laparoscopic repair is the best surgical approach for all diaphragmatic hernias. The non-resorbable sutures is still widely performed in case of small defects. The use of laparoscopic mesh has made easier the repair of big hernias. The laparoscopic fundoplication is still the gold standard of the treatment of hiatal hernias. The laparoscopic access allows the repair of both hernias without added morbidity. However, In the open technique the procedure should be reasonably discussed specially in elderly patients. Due to the risk of complications, most of the authors have recommended simultaneous repair for the two hernias even in asymptomatic patients [8].
Conclusions
Association between Morgagni and hiatal hernias type I is exceptional. Computed tomography (CT) of the chest and the abdomen is important for the diagnosis. Surgical treatment should be applied in Morgagni hernia complicated with strangulation. On the other hand, simultaneous treatment of hiatal hernia type I is non- consensual.
Conflict of Interest: None
References
[1] Modi M,
Dey AK, Mate A, Rege S. Strangulated Morgagni's Hernia: A Rare Diagnosis and Management. Case Rep
Surg. 2016; 2016:2621383. [2] Hassan
A, Alabdrabalmeer M, Alealiwi
M, Danan OA, Alshomimi S. Incidental Morgagni hernia
found during laparoscopic repair of hiatal
hernia: Case report & review of literature. Int J Surg Case Rep.
2019; 57:97-101.
[3] Zhou Z-L, Li H, Li
J-F, Liu Y, Wang C, Wang
J.
A Rare Case of Laparoscopic Repair of Simultaneously Occurring Morgagni and
Paraesophageal Hernias.
Ann Thorac Cardiovasc Surg. 2016; 22:112-5.
[4] Nasr A, Fecteau A. Foramen of Morgagni
Hernia: Presentation and Treatment. Thorac Surg Clin. 2009; 19:463-8.
[5] Lee SY, Kwon JN, Kim YS, Kim KY. Strangulated Morgagni hernia in an adult: Synchronous prolapse of the liver and transverse colon. Ulus Travma
Acil Cerrahi Derg. 2018; 24:376-8.
[6] Chaturvedi A, Rajiah
P, Croake A, Saboo S, Chaturvedi A. Imaging of thoracic hernias: types and complications. Insights Imaging.
2018;9(6):989- 1005.
[7] Fu S, Carton M, Ghaderi I, Galvani C. Robotic-assisted simultaneous repair of paraesophageal hernia and Morgagni hernia:
technical report. J Laparoendosc Adv Surg Tech 2018;
28:745-50.
[8] Patel AP, Samsami D, Lee C, Lakha A, Ehrenpreis ED. The waiting game: laparoscopic repair of dual Morgagni and paraesophageal hernias in an elderly, infirm
patient. J Surg Case Rep. 2019; 8: rjz225.
Citation: Ferjaoui W, Karouia S, Talbi G, Gabsi S, Bayar R, Khalfallah MT. Strangulated Morgagni hernia and sliding hiatal hernia: A rare association.
Jr.med.res.2020;3(1): 18-20. Ferjaoui et al ©
All rights are reserved.
Submit your manuscript: www.jmedicalresearch.com