Full Text Article Open
Access 
Case report
Isolated right adrenal metastasis from an invasive
ductal breast
carcinoma.
Taha Mohammed Hassan 1*, Al Emadi Mohammed Abdullah 1, Lotfy Mohammed
1, Mustafa Mohamed Naser 2, Omar Amany Mohammed
Rabie 3, El
Mahdi Hoda Saleh 3.
|
1: Department
of
surgery 2: Department of radiology 3: Department
of pathology Al Emadi Hospital Doha, Qatar. *Corresponding author Correspondence to: Dr.taha@alemadihospital.com.qa Publication data: Submitted: April 23,2019 Accepted: June 27,2019 Online: October 15,2019 This article was subject to full
peer-review. This art This is an open access article distributed under the terms of the Creative Commons Attribution Non- Commercial License 4.0 (CCBY-NC) allowing to share and
adapt. Share: copy and redistribute the material in any medium or
format. Adapt: remix, transform, and build upon the licensed material. the work provided must be properly cited and cannot be used for commercial purpose. |
Introduction Invasive ductal carcinoma (IDC) is the most
common histopathological type of breast cancer,
accounting for up to 85% of all invasive breast carcinomas [1]. It spreads usually to the bone first.
Solitary metastasis is commonly located in the lung, liver or brain
[2]. Adrenal
glands locations are extremely rare [3]. We report
a case of isolated metachronous right adrenal metastasis, diagnosed
four years after breast IDC management. The aim is to highlight clinical, diagnostic and therapeutic characteristics of this entity. Case presentation We report
a case of 53 years old female
referred to surgery for right adrenal mass.
On her history
we noted a previous tumorectomy
followed by chemo and radiotherapy
for right breast invasive ductal carcinoma moderately differentiated Not Otherwise Specified (IDC-NOS). The
TNM staging of the tumor was T2 NX M0. On the four-year follow-up consultation, an incidental right suprarenal tumor was detected by abdominal ultrasound. CT and MRI scan
(Figure 1), confirmed the presence of a 5x7
cm right adrenal
gland mass.
Endocrinological workup revealed that the tumor was not secreting. The patient underwent Laparoscopic Adrenalectomy which had to be converted to open, from which the patient made uneventful recovery. Gross examination revealed firm capsulated
right adrenal mass, measuring 9 x 7 x 3 cm and about 123.5 grams
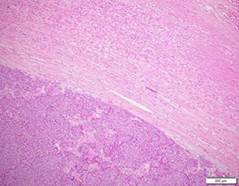
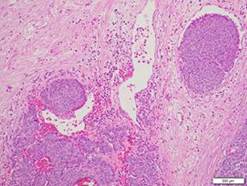
in weight with cut sections showed heterogenous cystic appearance. Microscopic examination revealed infiltration by sheets, clusters and cords of malignant cells
(figure 2a) with enlarged nuclei,
prominent nucleoli and frequent mitosis. The tumor
reached the surrounding fat with
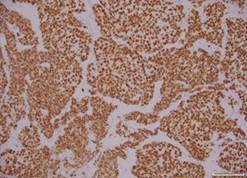
focal vascular invasion (figure 2b).Immunohistochemical staining revealed that tumor
cells expressed diffuse positive staining with ER (2+ in 80% of tumor cells)
(figure 4a), PR (2+ in 2% of tumor
cells), GATA3
(figure 4b), E-cadherin, BCL-2, HER-2 is equivocal (2+) and Ki67 proliferation index was 30%.
Histopathological confrontation of both
adrenal and breast
specimens revealed identical morphological and immunohistochemical features and was consistent with metastatic mammary carcinoma. Thereafter, the patient received
6 cycles of chemotherapy followed by hormonal therapy and kept a regular follow up until
now. |